
Moderate consumption of alcohol by adults is fundamentally low-risk.
Decades of clinical research including large cohort studies of all-cause mortality, everyday clinical observation and people’s experience show convincingly that sensible use of alcohol in social situations is well tolerated and holds only small absolute risk of harm.
We all also know that some people drink excessively every day or episodically and can suffer substantial physical damage that impairs and shortens their lives and adversely impacts those around them. Heavy consumption is not safe.
So, if we are drinking, how do we achieve moderation and avoid the pitfalls of excessive alcohol? What are reliable guidelines?
US Dietary Guidelines Allow for Alcohol in “Moderation”
The US departments of agriculture and of human services revise and publish Dietary Guidelines for Americans (DGA) every five years. They have for decades reflected research-backed conclusions that alcohol in moderation is safe. For example:
DGA 2000: “If you drink alcoholic beverages, do so in moderation.”
DGA 2005: “Those who choose to drink alcoholic beverages should do so sensibly and in moderation—defined as the consumption of up to one drink per day for women and up to two drinks per day for men.”
DGA 2020: “Adults of legal drinking age can choose not to drink, or to drink in moderation by limiting intake to 2 drinks or less in a day for men and 1 drink or less in a day for women, when alcohol is consumed.” This is the consumption standard adopted also by the National Academies of Sciences, Engineering and Medicine in their report in advance of the 2025 DGA recently released.
The 2011 Canadian Low-Risk (Moderate) Drinking Guidelines
I strongly support the low-risk drinking guidelines (LRDG) publicized by the Canadian Centre on Substance Use and Addiction (CCSA) in 2011. I believe this thorough and well-presented behavioral guidance document is accurate and provides more practical details about moderate drinking than the DGA. What are the LRDG specifics?
- Women should reduce long-term risk by drinking no more than 10 drinks per week and no more than 2 drinks per day. In addition, have at least 2 nondrinking days each week to minimize tolerance and habit formation.
- Men should reduce long-term risk by drinking no more than 15 drinks per week and no more than 3 drinks per day. Have at least 2 nondrinking days each week to minimize tolerance and habit formation.
- To reduce short-term risks, women should not take more than 3 drinks in any day and men more than 4 drinks. Such occasions should be accompanied by food and preferably by alternating with nonalcoholic drinks.
- Don’t drink when operating vehicles or machinery, if pregnant or planning to get pregnant or when breastfeeding, making important decisions, or in other high-risk situations. Youth should not start drinking till late teens.
Practical Additional Suggestions:
- Eat food when you drink alcohol. Absorption is slower, peak alcohol blood concentration is lower, risk of inebriation and discoordination is lower, and overdrinking is less likely.
- When drinking wine with dinner, wash the food down with water then sip the wine. That helps with volume control.
- Be especially careful when drinking spirits. It’s easy to over-imbibe substantial amounts of Scotch or vodka, but much harder to do that with beer or wine.
- Many medications interact badly with alcohol. Pay attention to drug labels or ask your pharmacist or physician.
- Older adults of either sex should be cautious about drinking close to the LRDG maximums. Lower muscle mass and slower metabolism promote higher alcohol levels with increased risk of falls.
What About the Canadian Guidelines That Scared Us in 2023?
I didn’t forget about the report released in January 2023 when the same Canadian Centre on Substance Use and Addiction publicized Canada’s Guidance on Alcohol and Health: Final Report. This report was funded by Health Canada, as were the 2011 LRDG guidelines I discussed earlier. Health Canada is the equivalent of our department of health and human services.
I know that many adults have been concerned and confused since this 2023 report was widely publicized in the media and fearful that they were harming themselves even with minimal amounts of alcohol. That fear is misplaced, and this particular report can safely be ignored. It has even been ignored by Health Canada, the government agency that had commissioned it. I discuss the details of its demise and why it was wrong below.
Why Are Recommended Alcohol Limits Lower for Women?
Recommended alcohol limits are lower for all women for physiological reasons related to alcohol metabolism (breakdown and dispersion). These include women’s much lower levels of the enzyme gastric alcohol dehydrogenase, which initiates alcohol metabolism in the stomach before alcohol is even absorbed into the blood.
Also, tissue dispersion of alcohol is mainly into muscle and water and not into fat. Women biologically have a higher body fat proportion than men with accompanying lower muscle and water content (the “distribution space”). This structural difference leads to higher blood alcohol levels in women for a given amount of alcohol.
Finally, women in general are smaller, sometimes substantially so, but larger and more muscular women’s ability to metabolize alcohol may well be similar to that of smaller men. Biology is complicated. That’s why guidelines, not rules.
Be Sure You Are Actually a Moderate Drinker
Data from all-cause mortality studies support the benign nature of moderate alcohol consumption. The data appear robust at the level of 1-2 daily drinks for men and one for women. They are good though not so securely at the level of 3 daily drinks for men and 2 for women.
Inherent uncertainties pervade alcohol consumption data, both because we are all terrible witnesses to our actual alcohol intake and because there are so many confounding behaviors associated with alcohol use (smoking, nutrition, socioeconomic status, multiple simultaneous diseases) that affect observed health and mortality data in any study. So, no one should believe that there are neat demarcations between 1 drink daily versus 2 versus 3, etc. as reported.
Check yourself against the LRDG consumption standards. Multiple studies have established that most everyone underreports their alcohol consumption by at least 25-50%. Not because we are inherently devious, just human.
Measure your spirit drinks for a while to see what your pour of Scotch or bourbon actually is. For reference, researchers define one standard drink as 5 oz wine (12% ABV), 1.5 oz spirits (80 proof or 40% ABV) or 12 oz beer (5% ABV) where ABV stands for alcohol by volume. Check the total volume. Were your 2 shots of vodka 3 oz or 4 oz? Or more? Count how many glasses of wine and the amounts you pour or cans of beer (12 oz or 16 oz?) you really have in an evening.
You could be drinking much more volume than you realize and could be exceeding the top range for low-risk moderate drinking. If you do this with any regularity, you are a heavy drinker where the health risks increase rapidly.
The best protection against slipping into heavy drinking is to keep any daily consumption of alcohol to less than the suggested daily maximum, and to keep to none or minimal drinking 2 days per week or more. Somewhat like driving in the middle lane on the highway. You can drive in the breakdown lane by consuming the daily maximum each day, but it’s risky and much easier to hit the guard rail from there than from the middle lane.
Recapping the Damage From Heavy Drinking
Heavy drinking, whether continuous or episodic, will damage your body. What exactly is “heavy drinking?” Most authorities consider heavy drinking to be the regular ingestion of 3 or more alcoholic drinks per day by an adult woman or 4 or more drinks per day by an adult male. Episodic or binge drinking is 5 or sometimes many more drinks by a man or 4 by a woman in a single day.
Chronic heavy drinking produces alcoholic liver disease, increased cancers of the GI tract and breast, cardiovascular disease including hypertension, atrial fibrillation and stroke, as well as accidents and violence. Not to mention the social damage from family disruptions and job loss.
Binge drinking, even if episodically done, is comparably damaging to the body as is steady heavy drinking. A binge drinking episode, moreover, can acutely result in death from accidents, vomiting and aspiration, respiratory depression, cardiac arrhythmias and other horrors.
In my five decades of clinical experience I observed that the severest forms of alcoholic liver disease, such as cirrhosis and bleeding varices, typically derived from alcohol use disorder (AUD) with extraordinary alcohol intake (think 1 pint to a quart of vodka daily), but it is also clear that voluntary heavy drinking as just described will cause unpleasant medical trouble with high probability.
Research Support for Moderate Drinking as Low Risk
Decades of research support moderate alcohol consumption as part of a healthy lifestyle. Examples include large-scale multiyear nutritional studies of populations following a Mediterranean diet where red wine was routinely drunk at dinner and heart attack rates were much lower. Social science studies confirming the benefits of moderate alcohol in promoting social interactions and interpersonal satisfaction. And all-cause mortality studies of alcohol users compared to nonusers or never users of alcohol, which repeatedly show lower mortality rates with modest alcohol use, and no increase in mortality from alcohol till amounts well into the heavy use category. Let’s review some specifics.
Nutritional Data Support for Moderate (Low-Risk) Drinking
The relative safety of moderate drinking is strongly supported by dietary research since at least the 1990’s.
Major nutritional studies of that decade focused on the Mediterranean diet, as observed in Spain, Italy, Greece and adjacent countries, which was repeatedly shown to reduce heart disease. This diet is rich in olive oil, vegetables, whole grains, fish and nuts, with limited red meat and quite unlike the American diet that is heavily weighted toward red meat, dairy and carbohydrates. A glass or two of red wine with the evening meal is frequently an integral part of the Mediterranean diet experience.
One foundational study was the Seven Countries: A Multivariate Analysis of Death and Coronary Heart Disease (Harvard University Press, 1980), a long‑term observational study that linked Mediterranean dietary patterns — including habitual wine consumption — to lower coronary mortality.
And as recently as February a new PREDIMED nutritional follow-on study, Wine consumption, Mediterranean diet, and cardiovascular risk in two Spanish cohorts, showed lower cardiovascular and all-cause mortality in wine drinkers who adhered to the Mediterranean diet with nightly red wine, adding to the data that red wine may reduce mortality.
Social Benefits From Moderate Alcohol
While we all are aware of the personal and societal damage caused by excessive drinking and alcohol abuse, social scientists have also examined people using alcohol in moderation. There, studies have shown benefit from moderate alcohol use in group bonding, sociability and social cohesion. Group sociability in turn has known benefits for personal satisfaction, stress reduction, and probably on longevity. After all, people are more than the sum of their organs and diseases: we are social beings. Such findings are not a reason to start drinking if you don’t but do support moderate social alcohol having benefits for adults.
Lower All-Cause Mortality With Moderate Alcohol
Evidence that moderate alcohol use is associated with lower all-cause mortality, as well as lower heart attack deaths, is strong and reproducible. All-cause mortality studies are readily understandable to non-statisticians and are exactly the outcomes data that many people would like to know.
For such a study, you follow a large group of people who self-report how much alcohol they do or do not drink, observe mortality events over perhaps 5 years then statistically adjust for major socioeconomic differences, cigarette smoking and other relevant variables.
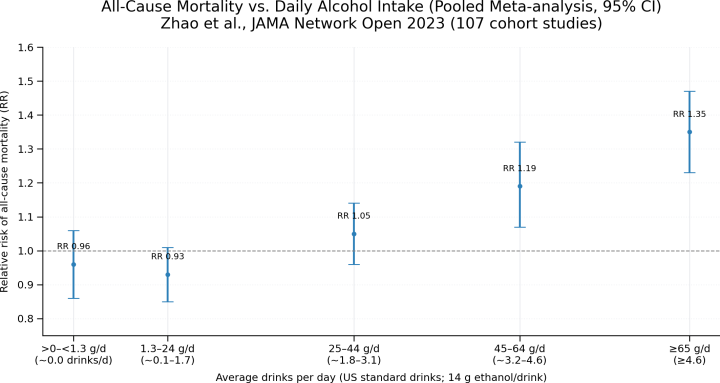
Multiple such all-cause mortality studies of drinkers carefully compared to true never-drinkers continue to show reproducibly lower mortality rates for people who have one drink daily compared to never drinkers. The mortality rate rises to baseline (equal to never drinkers) at 2 drinks, and to minimally higher at 3 drinks, often producing a J-shaped mortality curve. This point was specifically discussed in the 2011 Canadian CCSA report on low-risk drinking guidelines (LRDG). Note that heavy drinking starting at 4 drinks daily is associated with steadily increasing mortality. The included graphic from a recent JAMA article clearly demonstrates the flat to slightly J-shaped mortality curve with increasing rates at 4 or 5 daily drinks.
Statisticians have for years often fought over the validity of the control group of non-drinkers in all-cause mortality studies, because many nondrinkers actually were former drinkers who got into trouble with alcohol or who don’t drink because of baseline poor health. For the most part, modern all-cause mortality studies work to rigorously identify never-drinkers with normal health profiles as the control group, so that current all-cause mortality studies are on a solid basis.
The National Academies of Sciences, Engineering and Medicine (NASEM) performed just such a carefully constructed all-cause mortality meta-analysis, published in December 2024, in preparation for the latest US Department of Agriculture Nutritional Guidelines. It reaffirmed slightly decreased mortality with light-to-moderate drinking (1-2+ daily drinks) before rising to the baseline of nondrinkers. As usual, heavy alcohol use showed typically increasing mortality. The slight mortality reduction remains contentious. But for me, the key takeaway is the absence of any mortality increase in the moderate drinking range.
Brief Summary on Moderate Drinking
Alcohol is embedded in our culture. Half of American adults had at least one drink within the prior month while two-thirds drank at least some alcohol in the prior year. People enjoy the social use of alcohol. Restaurants depend on alcohol for their economic survival. Our country prohibited alcohol with the 18th amendment that went into effect in 1920. It lasted only 13 years till repeal and was widely ignored while in effect.
Extensive research over many decades shows that social consumption of alcohol in moderation is fundamentally safe. Not no risk, but certainly low risk. An individual may have a history, or genetics, or certain medical conditions where alcohol would be a more meaningful risk and even moderate drinking should be avoided. And certainly no one needs to drink if they don’t care to. But for the general population the reproducible all-cause mortality studies are compelling: Moderate alcohol consumption does not increase mortality.
The 2011 low-risk alcohol drinking guidelines from the Canadian Centre on Substance Use and Addiction (CCSA) were well researched, well written, practical and supported by the data. They still are accurate. I expanded on them with further practical suggestions, since to enjoy the benefits of low-risk alcohol you must be sure you really are drinking only in moderation. Stay in the middle lane. Don’t push the upper consumption guidelines. Heavy drinking or abusive drinking are seriously harmful.
I hope this updated and amplified guidance is helpful to you.
Epilogue: Why the 2023 Canadian Alcohol Guidance Was So Wrong
Let me briefly detail why the CCSA 2023 alcohol guidance should be and was scientifically disregarded.
In essence, this report purported to demonstrate that any amount of alcohol is inherently dangerous and that no one should consume more than 1 or 2 alcoholic drinks per week or risk increased dangers of early mortality. This evaluation was widely publicized in the media, largely without careful investigation, and scared many of us. Essentially, this report indicated that most every person who drinks any alcohol was drinking dangerous amounts.
First, that assertion didn’t make any sense to me because it conflicted with my fifty years of primary care experience and detailed familiarity with who drank, how much, and what became of them medically and it conflicted as well as with the many well-executed all-cause mortality studies.
Second, the 2023 CCSA report did not collect any new data. Instead, it was an enormous and complex set of statistical calculations (meta-analyses) of other published clinical studies on the relationship of alcohol use to mortality rates from about 14 different diseases, mostly cancers, which represent only a fraction of overall mortality. The included disease-specific alcohol studies in turn were themselves meta-analyses of individual studies involving those particular cancers.
Third, these results were combined to calculate the “alcohol-assisted fraction” of “global burden of disease” related to alcohol and then somehow summed up and projected via elaborate assumptions and computer modeling to an overall mortality rate related to alcohol use at different levels, without a crosswalk to actual mortality rates.
Key elements of how the authors did the modeling and how they corrected for confounding data and uncertainty were not clearly explained, even after reading the voluminous appendices. Ultimately, how the investigators came to specific conclusions cannot be verified from their publication.
Fourth, the study reported risk levels down to 1 or 2 or 3 or 4 or 5 drinks per week. But there are no consumption studies that track alcohol intake that low in relation to any disease. The authors said they did linear extrapolations from the higher consumption data down to 1 or 2 drinks per week to construct the purported low-consumption data. There is no valid statistical basis to do this and hence no valid way to say, as they did, that consumption of more than 1-2 drinks per week is dangerous and associated with early mortality. Nor is there a basis for their contention that no threshold amount of alcohol consumption exists that could be low-risk.
For all these reasons, this 2023 CCSA study, which provoked such concern and even fear in many adults, can be and should be rejected, as it was by multiple senior scientific groups such as the National Academies of Sciences, Engineering and Medicine, whose 2024 all-cause mortality study discussion (mentioned earlier) strongly cautioned against the CCSA data modeling approach, and the Canadian Medical Association Journal.
Most important, and definitive to me, the study was disowned and killed by Health Canada, who birthed it. Requiescat in pace
Have a Wonderful Spring.
If you drink alcohol, follow the 2011 Low-Risk Drinking Guidelines. Moderate consumption of alcohol by adults is low-risk and fundamentally safe.